In the ever-evolving landscape of healthcare, maintaining a strong culture of safety is paramount. American Data Network shines a spotlight on the benefits of safety culture surveys. Specifically, we promote the value of the AHRQ (Agency for Healthcare Research and Quality) Culture of Safety Survey. This tool is instrumental in assessing and improving patient safety culture in healthcare settings.
Hospitals owe it to their patients and staff to function as HROs, or High Reliability Organizations. HROs are safe, error-free environments with a reliable and consistent quality of care. Such organizations have the data to back up their success, including positive patient outcomes and high staff retention.
https://www.americandatanetwork.com/wp-content/uploads/2024/02/healthcare-workers-sitting-modern-hospital.jpg6671000Dalana Pittmanhttps://www.americandatanetwork.com/wp-content/uploads/2020/01/American-Data-Network-Logo-24-min.pngDalana Pittman2024-01-31 01:57:152024-02-01 03:36:48HRO Trait: Sensitivity to Operations – The Key Concepts and Benefits
A Good Catch Campaign fosters a growing culture of safety by encouraging the recognition and reporting of risk before a patient is harmed. This guide will help you follow the roadmap created by American Data Network Patient Safety Organization for its 45-Hospital Good Catch Campaign.
https://www.americandatanetwork.com/wp-content/uploads/2023/05/Magnifing-glass-and-documents-with-analytics-data-lying-on-table-2.jpeg6671000Stephanie Ioriohttps://www.americandatanetwork.com/wp-content/uploads/2020/01/American-Data-Network-Logo-24-min.pngStephanie Iorio2024-01-30 16:47:002024-06-05 10:07:16How to Implement a Hospital Good Catch Program
The intersection of healthcare and technology has paved the way for groundbreaking advances in patient care. As part of this dynamic shift, specialized registries, like the NCDR – TVT (Transcatheter Valve Therapy) Registry, have emerged, playing a pivotal role in optimizing outcomes and enhancing our understanding of specific medical procedures. Today, we shine a spotlight on this registry and its real-world impact.
Explore practical, ready-to-implement strategies based on real-world examples for the 2024 Hospital National Patient Safety Goals. This concise guide bridges theory and practice, simplifying the implementation of these crucial safety standards in hospitals.
Patient Safety Event Reporting: A Guide to Improving Patient Safety & Outcomes
Navigating the intricacies of patient safety event reporting is crucial for every healthcare facility. Dive into this comprehensive guide to learn how effectively capturing and leveraging event data can promote safety and improve quality of care.
⏰ 27 min read
Published on October 16, 2023
Listen to this article
How to use this Patient Safety Guide
This comprehensive guide is crafted to assist managers and directors of patient safety and risk in their mission to enhance patient safety and outcomes, serving as an all-encompassing resource that delves into the pivotal elements of patient safety while hyperlinking to a trove of actionable resources within each section. Designed to be both informative and practical, it can act as an invaluable primer for individuals newly introduced to the realm of patient safety. However, its primary purpose is to serve as a bookmark-worthy companion, aiding professionals as they navigate through various facets of patient safety within their facilities and seek pertinent resources tailored to address their current area(s) of focus.
Patient safety event reporting is not just a regulatory mandate; it is a moral imperative that underpins the trust patients place in healthcare institutions. It encompasses a vast array of safety events, ranging from unsafe conditions or near misses that have yet to cause harm to serious adverse events that can have significant consequences. The rich data harvested from these reports are vital in driving initiatives that elevate the standard of care and safeguard a patient’s well-being. In this guide, we delve deep into the intricacies of patient safety event reporting, laying down a roadmap to foster cultures that value transparency, learning, and collaborative improvement.
Before we explore patient safety event reporting in detail, let’s define some basics first for healthcare workers just beginning their foray into patient safety.
What is a patient safety event?
A patient safety event is any unplanned or unexpected event that results in, or could have resulted in, harm to a patient. Patient safety events can range in severity from minor incidents, such as a patient fall, to more serious events, such as medication errors or wrong-site surgery.
But a well-designed patient safety event reporting system should capture more than just the events that reach the patient. The Agency for Healthcare Research and Quality (AHRQ) has provided standardized definitions and formats used across healthcare settings that are called the Common Formats for Event Reporting (CFER).
CFER enables reporting of:
Incidents: patient safety events that reached the patient, regardless if there was harm involved
Near Misses (Close Calls or Good Catches): patient safety events that didn’t reach the patient
Unsafe Conditions: circumstances that increase the probability of a patient safety event occurring
Why is patient safety event reporting important?
Patient safety event reporting is important for a number of reasons. First, it helps healthcare organizations to identify the root causes of patient safety events. This information can then be used to develop and implement corrective actions to prevent similar events from happening again.
Patient safety event reporting also helps healthcare organizations track trends. This information can be used to identify areas where improvement is needed and to evaluate the effectiveness of corrective actions.
Additionally, event reporting helps to create a culture of safety in healthcare organizations. When healthcare workers feel comfortable reporting patient safety events, they are more likely to do so. This leads to more accurate and complete data, which can be used to improve patient safety more effectively.
Section I: The Cornerstone of Effective Safety Event Reporting – Establishing a Just Culture
Objective:
To create an environment where individuals are encouraged to report safety events without fear of punitive action.
Strategies:
Develop non-punitive reporting policies.
Facilitate open dialogues to address concerns and improve systems.
A “just culture” in healthcare is built upon the foundational belief that individuals should not be punished for mistakes attributed to systemic or process errors. In such a culture, reporting safety events becomes a norm rather than an exception, encouraging learning and growth. Let’s evaluate two pivotal strategies that help in establishing a just culture.
1.1.1 Develop Non-Punitive Reporting Policies
In a healthcare setting, where the stakes are notably high, establishing non-punitive reporting policies is crucial for fostering a culture of safety and accountability. This approach ensures staff members can report errors and near misses without fearing retribution.
Key Considerations:
Confidentiality: Ensure that reports can be submitted with attribution OR anonymously to protect the identity of the reporting individual, fostering a sense of security. (In ADN’s experience, 20% of patient safety events tend to be anonymous.)
Learning, not Blaming: Steer away from a culture of blame to one that emphasizes learning from incidents to prevent them in the future. Tactics to achieve this can be found in the Increase Event Reporting Toolkit.
Feedback and Follow-Up: Create mechanisms where the reporter receives feedback and sees tangible actions resulting from their reports, enhancing trust in the system.
Policy Formulation: Craft clear policies that delineate the non-punitive nature of the reporting system.
Awareness and Training: Organize workshops and training sessions to embed the non-punitive policy into the daily workings of the healthcare institution.
1.1.2 Facilitate Open Dialogues to Address Concerns and Improve Systems
Open dialogues serve as crucial platforms where concerns are expressed and solutions are developed. They demonstrate a commitment to transparency and ongoing improvement.
Key Considerations:
Safe Spaces: Create environments where individuals can voice concerns without fear, fostering a culture of openness and trust.
Cross-Functional Teams: Encourage teams from various areas to come together, bringing diverse perspectives to the table and enhancing problem-solving.
Iterative Improvements: Ensure that dialogues translate into action, with a focus on making iterative improvements based on feedback received.
Action Steps:
Regular Forums: Establish regular forums for open discussions, where team members can discuss challenges and brainstorm solutions.
By nurturing a just culture through non-punitive reporting policies and open dialogues, healthcare institutions embark on a path of self-improvement and learning, where every safety event becomes a stepping stone towards a safer, more effective healthcare environment. This collaborative and open approach not only protects the dignity and morale of healthcare professionals but also translates into enhanced patient safety and positive outcomes.
Section II: The Mechanics of Safety Event Reporting
Understanding the mechanics of safety event reporting is foundational to improving patient safety and healthcare quality. In this section, we delve into the essential components and processes that facilitate effective reporting of safety events, near misses, and unsafe conditions. From identifying and categorizing safety events to designing a robust reporting system, we explore the strategies and best practices that foster accurate and insightful data collection. By establishing clear guidelines and promoting open communication, healthcare organizations can create a conducive environment for reporting and learning from safety events, ultimately driving positive change and enhancing patient care.
2.1 Identifying Safety Events
Objective
To delineate clear criteria for identifying safety events, including good catches and unsafe conditions, thereby encompassing a broad spectrum of scenarios from medication errors to surgical complications to an unsafe sharps disposal bin. This concerted approach ensures that all possible safety concerns — not just those that result in incidents that reach the patient — are identified, monitored, and managed appropriately to foster a culture of proactive safety.
Strategies
Create guidelines and checklists to aid in identifying safety events, good catches/near misses, and unsafe conditions.
Train healthcare providers in recognizing and reporting safety events promptly.
2.1.1 Create Guidelines and Checklists
In order to facilitate the comprehensive identification of safety events, the creation of detailed guidelines and checklists is pivotal. Event recognition is repeatedly one of the top barriers to reporting. The guidelines/checklist approach not only aids healthcare providers in recognizing a wider array of safety events but also promotes an environment where good catches and the identification of unsafe conditions are encouraged and rewarded.
Key Considerations:
Inclusivity: The guidelines should be inclusive, encapsulating a wide array of potential safety events.
Clarity: The checklists should be clear and concise to facilitate quick and efficient reporting.
Accessibility: Both the guidelines and checklists should be readily accessible to all healthcare providers.
Action Steps:
Collaborative Development: Engage a diverse group of healthcare providers in the development process to ensure a comprehensive set of guidelines.
Regular Updates: Ensure the guidelines and checklists are regularly updated to remain relevant and effective.
Training plays a pivotal role in ensuring the effective implementation of any new strategy or guideline. Hence, healthcare providers should be systematically trained to recognize and promptly report safety events, good catches, and unsafe conditions.
Key Considerations:
Comprehensive Training: Utilize holistic training that includes theoretical knowledge and practical demonstrations.
Scenario-Based Training: Utilize real-life scenarios for training to better equip healthcare providers in identifying safety events.
Continuous Education: Establish a continuous education program to keep healthcare providers updated with the latest knowledge and best practices.
Action Steps:
Development of Training Modules: Create detailed training modules with inputs from experts in the field.
Feedback and Improvement: Gather feedback post-training and make necessary improvements to the training module based on the feedback received.
Certificate Program or CE Credit: Introduce an in-house certificate program to encourage healthcare providers to embrace the training. This could even include incentives like extra vacation time, a celebration for new certificate recipients, etc. Additionally, the certificate could include continuing education hours for existing licenses or certifications.
By concentrating on identifying not only safety events but also good catches and unsafe conditions, healthcare organizations can cultivate a culture that is proactive in seeking to enhance safety at every opportunity. Committing to these strategies will contribute to creating safer healthcare environments, with every stakeholder playing an active role in maintaining safety.
The High Stakes of Event Miscategorization
In 2018, American Data Network Patient Safety Organization (ADNPSO) conducted a deep-dive analysis of the event type “Other.” Over a four-year period, this catchall category accounted for over 40% of events reported by ADNPSO members. Among the myriad of striking revelations,the death rate of incidents categorized as Other was 3 times higher than ALL remaining event categories combined.The results of the Other analysis proved so compelling that ADNPSO was selected to present at the National Association for Healthcare Quality (NAHQ) Conference.
Of the 500 random event narratives reviewed for the subcategory “Other Other” (top level category = Other; subcategory level also = Other), ADNPSO recommended that 70% (or 346) were miscategorized and should be recategorized to one of the more specific subcategories or event types.
If your team is using the 80/20 Rule (or Pareto Principle) to prioritize time and resources, events that are miscategorized and hiding in Other may be skewing your data, meaning you may not actually be focusing on the top priorities. Risk Managers should review and appropriately categorize events prior to closing them to produce a more accurate set of priorities. ADNPSO also recommends using miscategorizations as an opportunity to educate frontline staff and curb future errors.
Strikingly, nearly all of the Other events that resulted in death were miscategorized. Of the 500 random Other Other events reviewed, 7 resulted in death; and 6 of the 7 warranted recategorization to more specific subcategories such as Delay in Treatment, Code/Emergency or Medications.
2.2 Designing and Implementing a Robust Reporting System
Objective
To construct a reporting system that is readily accessible to all healthcare providers and structured to capture intricate details pertaining to safety events, ensuring a holistic view of the incidents, near misses, and unsafe conditions. This system aims to promote a culture of transparency and continuous improvement through the meticulous documentation and analysis of safety events.
Strategies
Prioritize User-Friendly Reporting for Frontline Staff
Ensure Integration of Feedback Mechanisms
2.2.1 Prioritize User-Friendly Reporting for Frontline Staff
Perhaps the most frequently cited barrier to reporting an event (see table below) is not enough time. Thus, a fundamental step in building a robust reporting system is the implementation of user-friendly report templates (also know as reporting forms) that encourage detailed documentation of incidents, good catches, and unsafe conditions. These forms should not only facilitate easy reporting but also help in capturing vital data that can be analyzed to improve patient safety. Striking a balance between capturing as much data as possible while being user-friendly is a challenge (but one that ADN has achieved given that an independent expert called ADN’s event reporting system the easiest for frontline staff of all the tools in the market). In fact, one ADN client conveyed they had their IT team set the shortcut icon on computers that links to ADN’s event reporting application to be a big red “E” because frontline staff call it “the ‘Easy Button’ because it’s so easy to report an event.”
Key Considerations:
Clarity: Ensure the form is clear and straightforward to encourage widespread usage.
Guided Inputs: Incorporate guided inputs, such as skip logic and prepopulated patient data fields, to assist providers in detailing incidents effectively.
Customizability: Allow the template to be customizable to cater to the diverse needs within the healthcare facility.
Action Steps:
Scrutinize Available Offerings: Scrutinize the user-friendliness of the reporting form to set the facility up for success. The ease-of-use of the event reporting system directly correlates to the quality and quantity of data you’ll get for data-driven decision making. In your evaluation of the event reporting products on the market, this should not be short-changed. (Consider using a prebuilt gap analysis tool to compare reporting tools.)
Pilot Testing: Conduct pilot tests to refine to obtain real-world feedback, identify friction points, and establish buy-in.
Training: Offer training sessions to familiarize healthcare providers with the new reporting template, ensuring ease of use and encouraging its utilization.
2.2.2 Ensure Integration of Feedback Mechanisms
For effective safety event reporting, it’s vital that event reporters, especially frontline staff, receive acknowledgment and feedback on their reports. This type of feedback reaffirms that their efforts in reporting were meaningful and had an impact. Creating a feedback loop centered on acknowledging and valuing the contributions of reporters is key. It not only assures staff that their reports are being reviewed and acted upon but also emphasizes the significance of every report in fostering a safer healthcare environment.
Key Considerations:
Feedback Channels: Prioritize channels where reporters receive timely feedback. This can include direct acknowledgment messages such as “thank you for reporting” and more detailed feedback when a report leads to further investigations or interventions. While functionalities like commenting and messaging are prevalent in 3rd party event reporting applications like ADN’s, in-house tools may lack these features. Assessing this disparity is crucial if considering an in-house tool.
Feedback Reinforcement: Apart from immediate acknowledgments, it’s essential to publicize instances where a particular report led to tangible improvements. This not only validates the reporter’s effort but also shows the organization’s commitment to continuous improvement. Daily safety huddles can be effective platforms for public kudos like this.
Action Steps:
Feedback Workshops: Regular sessions can be held to share broader insights gained from individual reports, and the subsequent improvements implemented. This can serve as a motivational tool for staff to understand the broader impact of their individual reports.
Incorporating feedback mechanisms focused on acknowledging the contributions of reporters ensures that healthcare organizations are building trust and promoting a culture of safety. This approach, emphasizing both immediate acknowledgment and showcasing broader improvements resulting from individual reports, guarantees a proactive, responsive, and engaged reporting environment. The ultimate goal remains the same: enhancing patient safety outcomes by valuing every report and every reporter.
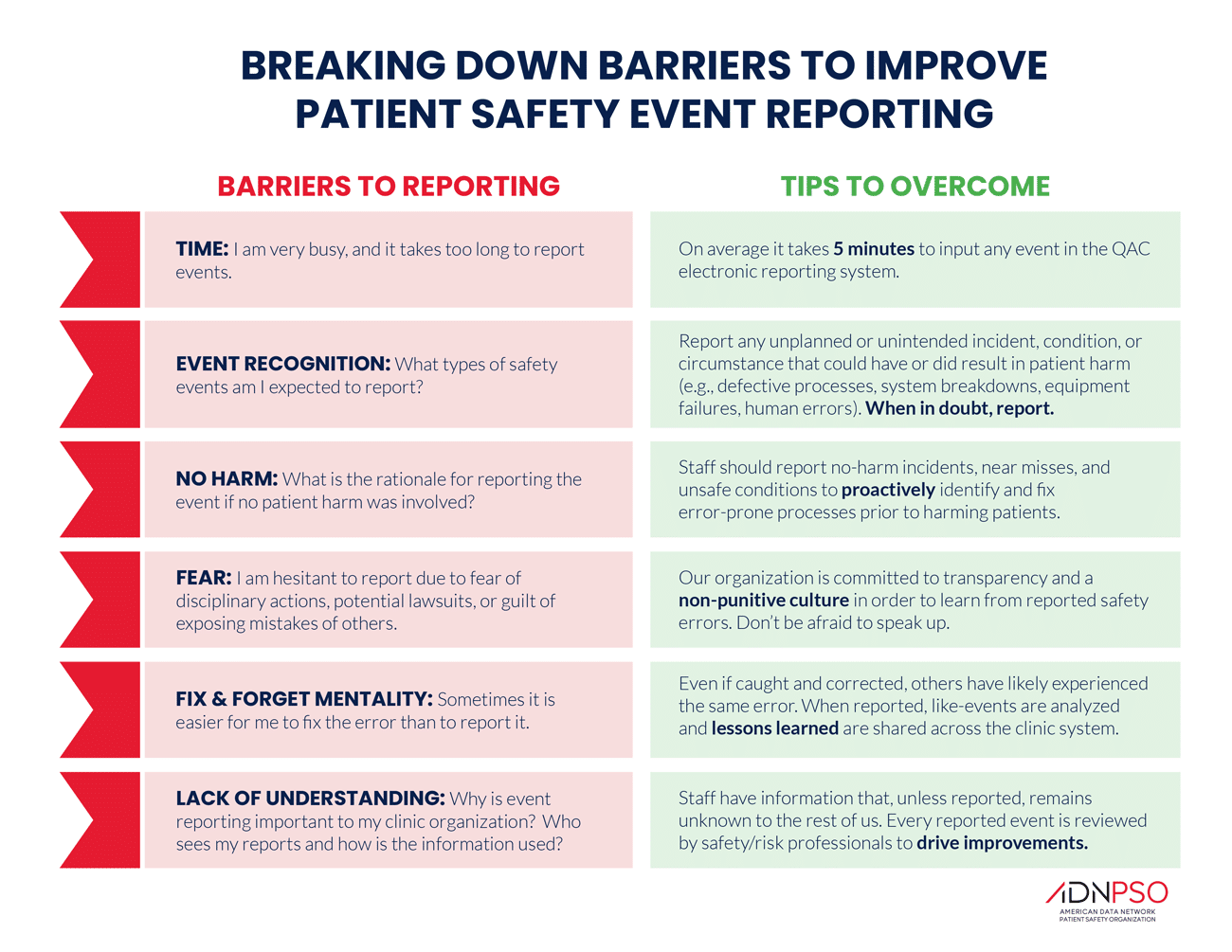
2.3 Overcoming Barriers to Event Reporting
Despite the importance of patient safety event reporting, there are a number of barriers that can prevent healthcare workers from reporting events. Fortunately, healthcare organizations can overcome these barriers if they’re clear-eyed and strategic. The table below identifies the most common barriers to event reporting in ADN’s extensive experience in patient safety as well as tips for how to overcome them.
Section III: Analyzing and Leveraging Data from Safety Reports
Effectively analyzing and using data from safety reports is crucial for enhancing patient safety and outcomes in healthcare. This section explores practical methods and strategies for collecting and interpreting this data to identify areas that need improvement. Transforming these insights into concrete actions is essential for ongoing improvement in safety protocols and practices. In this part of the guide, we’ll focus on how healthcare organizations can make the most of the information gathered to make real and lasting improvements in patient care and safety.
3.1 Data Aggregation and Analysis
Objective
To amass and scrutinize data systematically, extracting crucial insights to spotlight areas necessitating change. A deliberate and thorough analysis is pivotal in transforming raw data from safety reports into actionable strategies that foster heightened patient safety.
Strategies
3.1.1 Employing Sophisticated Data Analytics Tools
In the age data-driven decision making, healthcare data analytics stand as a beacon of insight, helping organizations chart their path forward. Using state-of-the-art data analytics tools, healthcare institutions can delve deep into the safety report data, identifying patterns, discerning trends, and highlighting critical areas of concern.
Key Considerations:
Tool Selection: Picking analytics tools that are well-suited to the unique demands and complexities of healthcare safety data.
User-Friendliness: Ensuring the tool interface is intuitive, enabling efficient and effective usage by the designated teams.
Data Security: Given the sensitive nature of healthcare data, prioritizing tools that ensure the utmost data security.
Action Steps:
Tool Evaluation: Conduct thorough assessments to select the most apt analytics tools for safety report analysis.
Training: Organize training sessions to acquaint teams with the tool functionalities, optimizing their analytical capabilities.
3.1.2 Establishing Multidisciplinary Teams
Data, while insightful, often demands a multifaceted perspective for comprehensive understanding. By bringing together experts from various disciplines, healthcare organizations can ensure a more holistic and enriched analysis of safety report data.
Key Considerations:
Diverse Expertise: Ensure the team comprises members with diverse backgrounds, from clinicians to data scientists.
Collaborative Approach: Foster a culture of open dialogue and collaboration within the team.
Continuous Learning: Promote ongoing education and training for team members to keep abreast of the latest analytical methods and healthcare safety trends.
Action Steps:
Team Formation: Select experts from various fields to form a multidisciplinary team.
Regular Meetings: Schedule regular meetings to discuss findings, share insights, and brainstorm solutions.
Feedback Mechanism: Establish a feedback loop within the team to ensure continuous improvement in the analytical process.
Through deliberate aggregation and analysis of safety report data, healthcare organizations are better positioned to identify areas of concern and craft targeted interventions. By leveraging sophisticated analytical tools and fostering multidisciplinary collaboration, the journey from raw data to actionable insights becomes a seamless, efficient process, anchoring patient safety at the core of decision-making.
3.2 Transforming Insights into Action
Objective
To harness the insights gleaned from patient safety analytics, driving forward initiatives specifically tailored to bolster patient safety. This transformation from data to actionable steps is paramount in ensuring that the lessons learned from safety events are constructively applied to the healthcare environment.
Strategies
3.2.1 Developing Actionable Plans Rooted in Data Insights
Translating insights into tangible action is a pivotal step in the patient safety journey. These insights, stemming from rigorous data analysis, provide a roadmap for crafting plans that directly address identified areas of concern in patient safety protocols.
Key Considerations:
Prioritization: Pinpoint the most pressing concerns identified through data analysis to address first.
Stakeholder Engagement: Involve relevant stakeholders, from frontline medical staff to hospital administration, in the planning process.
Resource Allocation: Determine the time, personnel, and/or financial resources required to implement the plan effectively.
Action Steps:
Brainstorming Sessions: Organize sessions with multidisciplinary teams to develop actionable plans based on identified insights.
Plan Documentation: Ensure every plan is meticulously documented, outlining steps, responsible parties, timelines, and expected outcomes.
Roll-out: Launch the plan across the organization, accompanied by adequate training and support for involved personnel.
The Hierarchy of Data Maturity: What Level Are You Really?
Over the years, many organizations to varying degrees of success have embarked on journeys to become “High Reliability Organizations.” But all healthcare organizations, whether they realize it or not, are on a Journey to Data Maturity. Some facilities are more clear-eyed than others about this concept while some may not realize they have stalled on this journey. So ADN developed a tool, the “Hierarchy of Data Maturity”, to help organizations honestly assess their approach to data and benchmark their current actual performance against the goal of reaching the promised land of data maturity.
The dynamic nature of healthcare demands that any implemented initiative be continuously monitored and refined. By establishing feedback loops, healthcare organizations can gauge the effectiveness of their initiatives, pivoting and refining based on real-world feedback.
Key Considerations:
Feedback Collection: Institute methods to actively gather feedback from healthcare providers and patients.
Data Integration: Merge feedback data with existing safety report data to provide a comprehensive picture.
Rapid Response: Ensure the capability to swiftly act upon feedback, making necessary adjustments to initiatives.
Action Steps:
Feedback Channels: Implement varied channels, from surveys to focus groups, to gather feedback on the new safety initiatives.
Regular Review: Schedule periodic review meetings to discuss the feedback received and assess the initiative’s impact.
Iterative Improvement: Based on feedback and review findings, make iterative improvements to the patient safety initiatives, ensuring they remain aligned with the evolving healthcare landscape.
In the ongoing effort to improve patient safety, turning data-driven insights into actionable strategies is fundamental. Through careful planning based on genuine insights and creating environments rich in feedback, healthcare organizations can continually evolve and adapt, keeping patient safety a top priority in their efforts.
Case Studies – Lessons from the Field
In the dynamic landscape of healthcare, a robust patient safety event reporting system stands as a cornerstone for enhancing the quality of care and safeguarding the well-being of patients. The ability to meticulously capture, analyze, and respond to safety events is not just a regulatory requirement but a catalyst for transformative change within healthcare institutions. A well-orchestrated reporting system serves as the eyes and ears of a hospital, unveiling hidden patterns and trends that might otherwise go unnoticed.
The significance of uncovering these hidden patterns is multifaceted. It enables healthcare providers to proactively identify vulnerabilities, mitigate risks, and implement corrective measures, thereby fostering a culture of continuous improvement and patient-centered care. From recognizing trends in falls during shift changes to detecting an increase in needle sticks, the revelations brought forth by a comprehensive reporting system are instrumental in driving proactive interventions and enhancing patient safety.
In the following case studies, we explore real-world scenarios where hospitals have leveraged the power of a strong patient safety event reporting process to uncover hidden patterns and trends. These narratives illustrate the transformative impact of such systems in identifying areas of improvement, implementing effective solutions, and ultimately elevating the standard of care provided to patients. Through these stories, we aim to shed light on the pivotal role of safety event reporting in shaping a safer and more resilient healthcare environment.
Case Study #1: Hospital Uncovers Culprit of Uptick in Staff Needle Sticks
The Director of Risk Management & Compliance of a Louisiana hospital relayed a tangible example of how they used ADN’s Dashboards to unearth a trend that was quickly diagnosed and resolved. “We noticed an uptick in staff needle sticks. Upon investigating, we learned that Materials Management changed supply companies. Using the dashboards, we were able to associate the uptick with the vendor change and ultimately we went back to the previous company.”
Without real-time dashboards like in ADN’s patient safety event reporting application, according to the risk management director, it likely would have taken days or weeks longer for the hospital to identify the root cause, resulting in many more unnecessary needle sticks that can carry serious consequences.
Case Study #2: The Journey from Paper Reports to Digital Insights
For one Hawaii hospital, transitioning away from a paper-based process to ADN’s electronic event reporting application was been transformative to their ability to act swiftly on event data.
The Quality & Performance Improvement leader recalled a recent event in which her team’s newfound speed was unmistakable. “We had an event where a patient fell and was injured while leaving our facility. I got an application alert about it immediately. When I talked to our manager, she showed me the place where the fall happened. The patient came down the steps but didn’t see the curb, even though it was painted yellow, and fell off the curb and landed in the parking lot.”
The team immediately summoned the maintenance crew and tasked them with building a railing that would enforce the use of the wheelchair ramp and prevent stepping off the curb. “So, within literally two days, we had a railing built where that curbing was located. Whereas if we had still been using paper reports, we may not have known the fall happened until longer than it took us to get the fix,” she said.
Six months after transitioning to ADN’s application, the team achieved a 9% decrease in falls from their enhanced ability to analyze and react to fall-related events, near misses, and unsafe conditions.
Case Study #3: Uncovering Hidden Trends with Easier-to-Use Analytics
Another hospital transitioned to ADN’s event reporting application from a different vendor. Perhaps the biggest benefit to the Director of Quality & Risk Management was ADN’s more intuitive and easier-to-use analytics.
She relayed a very tangible improvement resulting from her enhanced ability to uncover patterns and trends that previously lay hidden. “ADN’s event reporting system made it very easy to look at the time of day that events were occurring. When analyzing falls per unit, we were able to identify that in one particular unit there was an increased number occurring at shift change,” she said. “We implemented an action plan to make sure staff were located in high-risk areas during this time. We were able to see an improvement in fall reduction in the unit. If there was a Time-of-Day report in our previous application, it obviously wasn’t easy to find.”
The director said another trend discovered through regular monitoring of the event analytics was an increased number of specimen events. “We identified an increase in the number of specimen events so we started a new collaborative on Specimen Collection and Identification. We had our second meeting today where we are flowcharting the process, and we’re going to initiate a LEAN project focusing on that process,” she said. “This collaborative originated from information collected through ADN’s easy-to-use analytics and staff who feel safe reporting events.”
Conclusion – The Road Ahead
Patient safety event reporting is a foundational element in enhancing healthcare outcomes. By implementing robust reporting systems, fostering open dialogue, and leveraging advanced technology, healthcare organizations can address and mitigate safety concerns effectively.
Real-world case studies highlight the tangible improvements that can be achieved through diligent reporting and analysis. By addressing challenges head-on and transforming insights into actionable strategies, organizations can contribute to a culture of continuous learning and improvement in patient safety.
The vision for the future of safety event reporting is one of evolution and adaptability, with a focus on collaborative learning and transparency. It is incumbent upon healthcare leaders to champion these values, driving forward the mission to improve patient safety and healthcare quality.
By adhering to these principles and strategies, the healthcare community can continue to make strides toward a safer and more accountable environment for all patients.
ADNPSO’s analysis of 116 clinics revealed only 3 events reported PER YEAR per clinic across a 3-year period, underscoring the urgent need for a focus on improving the culture of safety in the outpatient setting.
https://www.americandatanetwork.com/wp-content/uploads/2023/05/Side-view-of-young-female-surgeon-using-digital-tablet-in-front-of-computer-at-desk-in-clinic.jpeg6671000Stephanie Ioriohttps://www.americandatanetwork.com/wp-content/uploads/2020/01/American-Data-Network-Logo-24-min.pngStephanie Iorio2023-03-15 15:36:172023-06-14 10:05:1318-Month, 116-Clinic Initiative Reveals Outpatient Setting in Urgent Need of Focus on Safety Culture + FREE TOOLKIT & FULL REPORT