Healthcare News
Everything You Need To Know
We know you’re busy. So we research, curate and report healthcare news you need to know.

A report by NAHQ reveals major skill gaps among the healthcare quality and safety workforce. Use these 5 tactics to close these gaps at your facility.

Smartsourcing is a business strategy of shifting towards partnerships that focus an organization on its core competencies and core mission, and to then shed the processes that are not core to the organization’s mission to a partner.

Healthcare organizations on the leading edge of quality improvement are reinventing their approach to data, focusing less on adding ever more data to an information black hole and instead organizing more resources around producing insight from the data and, most importantly, acting on it to accelerate change. This doesn’t mean they neglect data collection. Rather, they’re smarter in how they collect it by leveraging a trusted smartsourcing partner to handle the more routine task of data collection so they can concentrate their precious and scarce personnel on more advanced roles like analysts and change agents. This whitepaper details how ADN clients calculate and perceive the return on investment of smartsourcing data abstraction to a trusted partner so they can make more intelligent use of their financial and personnel resources.

The Survey on Patient Safety CultureTM (SOPS®), developed by the Agency for Healthcare Research & Quality, helps hospitals, medical offices, and other healthcare organizations understand how providers and staff perceive aspects of their culture of safety.
Organizations use the SOPS Assessment tool to:
All your efforts to create a High Reliability Organization are for naught if patient safety is not embraced at every level, from system to individual. And the only way to quantify your patient safety culture, and to identify problem areas, is by asking.
One of the most vetted measurement tools for this is the Survey on Patient Safety CultureTM (SOPS®) developed by the Agency for Healthcare Research and Quality (AHRQ).
While the AHRQ survey tool has been available since 2004, in recent years it’s gained more attention with the focus from accreditation organizations like The Joint Commission (TJC) and public-scoring watchdogs like Leapfrog.

At the end of 2018, TJC amended its survey process expectations for Patient Safety Culture Assessment.
But AHRQ’s survey is not a one-size-fits-all process. The flexibility — how often to survey, who to survey, how to survey, and what to do with the results — recognizes the enormous variations in size and resources of patient-care organizations. But it also means a large number of decisions have to be made in-house.
Here are 6 best practices for your next SOPS to both fulfill accreditor and watchdog expectations and, more importantly, to make the process pay off in the form of an improved safety culture for your organization:
Many organizations have continued to feel the strain of the healthcare staffing crisis since the pandemic. So even if you have handled the survey process in-house in the past, your capacity to do so now may have changed. And if you haven’t administered a SOPS in recent years, you might be hesitant to add it to your plate given that AHRQ’s User Guide for Hospital SOPS Version 2.0 outlines a 10-week timeline for planning, creating, conducting, and analyzing the survey.
Some advantages to outsourcing are obvious: The process doesn’t interrupt your normal duties and projects, and you don’t have to reinvent the tools or train someone in-house for a process that only happens every other year.
Some are less obvious: The right outsourcing partner can help you (1) achieve much higher response rates that enrich the results, and (2) receive a more sophisticated and enlightening analytics report faster than you might otherwise. (Our team turns the report around in less than 30 days.)
AHRQ points out several benefits of using an outsourcing partner in the User Guide:
When considering these benefits and the fact that outsourcing is very affordable, it’s often worth a brief conversation before you go too far down the road of investing a lot of internal time and resources in administering the SOPS yourself.

The pitfalls of a poorly designed online survey are so numerous that AHRQ produced a webinar on best practices as a companion to the SOPS User Guide.
Online surveying has virtually replaced paper surveys for many good reasons: online surveys prevent participants from giving two answers to the same question; they can capture responses if the survey-taker fails to finish all questions; and, most appealing, online survey responses are automatically compiled, resulting in actionable results within days rather than months.
Design elements that really matter include a proper grid layout, alternating row shading to help respondents move smoothly through the answer options, easy buttons for moving back and forth through the questions, and a progress bar to encourage the user to complete the survey. Also crucial is developing a survey that is easy to complete on a mobile device, not just a desktop computer.
The ability to monitor responses in real-time is one of the great advantages of online surveying compared with paper surveys, but that advantage is wasted if no one is paying attention until the end of the survey period. A good outsourcing partner will monitor and update you frequently – ADN, for instance, provides response rates at least twice a week at the overall facility and individual department levels – so that targeted promotional efforts can be implemented in a timely manner via huddles or other staff meetings. Your response rate should not be a surprise ending.
Even a well-designed survey will have a low response rate without consistent, multi-channel efforts to promote, encourage, incentivize and remind employees and other desired respondents to start and finish the survey. That means emails, preferably from the CEO; posters in common areas, verbal reminders at routine staff huddles; links on your intranet; etc.
If partnering with ADN, we have a sequence of pre-written email templates with recommended distribution dates/times that have been proven effective.
Rewards for departments with the highest response rates are more effective than random individual winners. And the reward should reflect the value your organization places on patient safety: an extra day of vacation, a catered meal, or maybe both. Through experience, our team has learned some creative and motivating incentives that we share with clients.
With so much data from a facility-wide survey, the quality of your analytics report can mean the difference between a sea of raw data or a trove of distilled insight. Below are some best practices ADN recommends.
For more than 25 years, American Data Network (ADN), which is also the parent company to its Patient Safety Organization (ADNPSO), has worked with large data sets from various sources, aggregating and mining data to identify patterns, trends, and priorities within the clinical, financial, quality and patient safety arenas. ADN developed the Quality Assurance Communication (QAC) application, with which hospitals, clinics, rehabs, and other providers record and manage patient safety events. By entering events into ADN’s QAC application and submitting them to ADNPSO, information is federally protected and thereby privileged and confidential. These protections provide a safe harbor to learn from mistakes and improve patient safety.
Fall prevention in healthcare involves managing patients’ underlying risk factors and optimizing their environment to reduce the likelihood of an unplanned descent to the floor. Resources such as Fall Prevention Toolkits have been shown effective in reducing this type of patient safety event.
A hospital is an unfamiliar setting, and every patient is there because of an illness or condition that requires treatment. It’s a recipe that increases the likelihood of falls, one of the most common and most devastating events in any hospital setting.
While the rate of falls varies among hospitalized adult patients depending on the study, multiple studies indicate that 3-4 falls occur per 1,000 bed days.
A fall, especially by a geriatric patient, can be the start of a downward spiral as described by the team that did early research on the use of a fall prevention toolkit. A single fall can have compounding effects and result in fear of falling, reduced mobility, loss of function and greater risk of falls.”
That early research, published in the Journal of the American Medical Association in 2010, found a significantly reduced rate of falls in the hospital setting when a toolkit was added to usual care protocols. Over the next decade and funded through a grant by the Agency for Healthcare Research & Quality, that research team would go on to further refine their toolkit to help facilities prevent falls. And the toolkit resulting from all that work — Fall Tailoring Interventions for Patient Safety (Fall TIPS) — was recently released for free.
In another JAMA study including more than 37,000 patients published in 2020, the Fall TIPS toolkit was tested at Brigham and Women’s Hospital in Boston and 2 other facilities, finding that falls with injury were reduced by 34% while total falls decreased by 15%. Since then, more than 100 hospitals in the U.S. and internationally have used the toolkit.
When Fall TIPS was first developed, use of the nurse-led, evidence-based toolkit proved to reduce falls by 25% in acute care settings when implemented as part of electronic record-keeping. The Fall TIPS team then set out to create a “low tech” tool that offered the same benefits in preventing falls, the end result being an 11″x17″ laminated poster on which the personalized plan for each patient is marked.
In the EHR version, the patient’s risk factors and tailored interventions automatically populate the Fall TIPS electronic poster, which a nurse then prints and hangs in the patient’s room. While the integration into a facility’s EHR reduces the potential for error, it also requires the involvement of the IT team to set up. The lower-tech, laminated poster version, on the other hand, can easily be filled out with a dry erase marker and updated daily at the bedside. (A full list of the pros and cons of the paper and electronic methods can be found on the Fall TIPS site under the heading “Paper or Electronic?”)
Whether a high- or low-tech solution is implemented, the goal is to use bedside tools to communicate current and changing patient risk factors, so all stakeholders have access to the information needed to engage in prevention activities.
The human cost of falls is not the only cost. One-third of falls result in injury, and injurious falls can add a week or more to a hospital stay. The same JAMA study from 2020 found that the additional cost was $19,376 to $32,215. And these costs are not reimbursed by the Centers for Medicare & Medicaid Services because most (more than 90%) of falls are preventable.
When implementing a performance improvement tool like Fall TIPS, it’s always a best practice to start by ensuring you can track and measure success for communication to the team on the frontline as well as senior leadership. The best way to accomplish this is through a Patient Safety Event Reporting Application with real-time dashboards. If your tool has a dedicated Falls Dashboard like ADN’s application (see video below), evaluating falls data pre- and post-implementation of a tool like this is much easier.
At the patient level, Fall TIPS is a three-point plan of action:
The toolkit is easy enough to use that compliance was above 80% at the hospitals where it was first tested. So with administrative buy-in and training of patient-care staff, Fall TIPS can become a routine and effective part of patient care. (Subsequent research by the Fall TIPS team showed that a compliance rate of at least 80% is necessary to achieve a clinically significant reduction in falls.)
A poster in the patient’s room is the most visible tool in the toolkit (either the laminated version or the EHR printout). But implementation starts at the top with administrative support. That should include engaging any relevant committees and champions. Some organizations may already have a specific fall-prevention task force, or the appropriate body might be a general quality and safety council. Buy-in needs to come from within the existing organizational structure.
Implementation also includes analyzing existing fall-prevention protocols to see how much overlap there is with the best practices. The toolkit includes a tool to assess gaps in protocols, as well as an implementation checklist and training materials for champions and nurses. (To get started implementing Fall TIPS, click here.)
Whether using the high- or low-tech version of Fall TIPS, the result is a personalized assessment of the patient’s risk of falling and a personalized plan to address their specific risk profile.
Does the patient have a history of falls? Are they taking medications that might contribute to unsteadiness? Do they already use a cane or walker? Are they likely to get out of their bed or chair without summoning help?
Once the patient’s risk factors have been committed to the record, interventions to mitigate those risks can also be committed to the care plan. Is a bedpan appropriate, or should the patient be assisted to the toilet? How many helpers does the particular patient need? Is the risk of getting up unassisted so great that a bed alarm is required?
All of the risk factors and interventions should be discussed with the patient and with family members so that everyone involved understands the plan for preventing falls. In fact, whether the patient and/or family can verbalize the patient’s risk factors and the fall-prevention plan are part of the audit questions that internal champions must answer.
Patient and family feedback has affirmed that knowing the plan improves compliance and can help reduce the fear of future falls, a factor in the downward spiral of fall-prone patients.
Fall TIPS is not a one-size-fits-all plan for every patient, nor is it static for the individual patient. It can be customized as the patient’s condition changes. The patient’s risk factors and appropriate interventions should be re-evaluated daily. The poster features an assessment date so that every care provider can see how current the evaluation is.
A patient may, for instance, be at greater risk of falling and need different levels of assistance immediately after surgery than before. A change in medications may also change risk factors and the interventions needed. With training and consistent use, Fall TIPS can reduce the number of patient falls and reduce the number of injuries associated with falls that do happen.
To download and start using the Fall TIPS Toolkit, click here.
Learn more about how ADN’s Patient Safety Event Reporting Application can help you uncover trends and patterns about falls in your event data.

Voluntary Patient Safety Event Reporting is a method of collecting details and information about an incident, near miss or unsafe condition in hospitals and other care settings through an electronic or paper-based form submitted by frontline staff.
As research published in 2020 by the Journal of Patient Safety acknowledged, “A natural, human tendency when errors have occurred is to ignore or minimize the error. It takes a lot of work to build an environment that supports the opposite reaction: open and honest reporting of errors so they can be evaluated to contribute to organizational learning.”
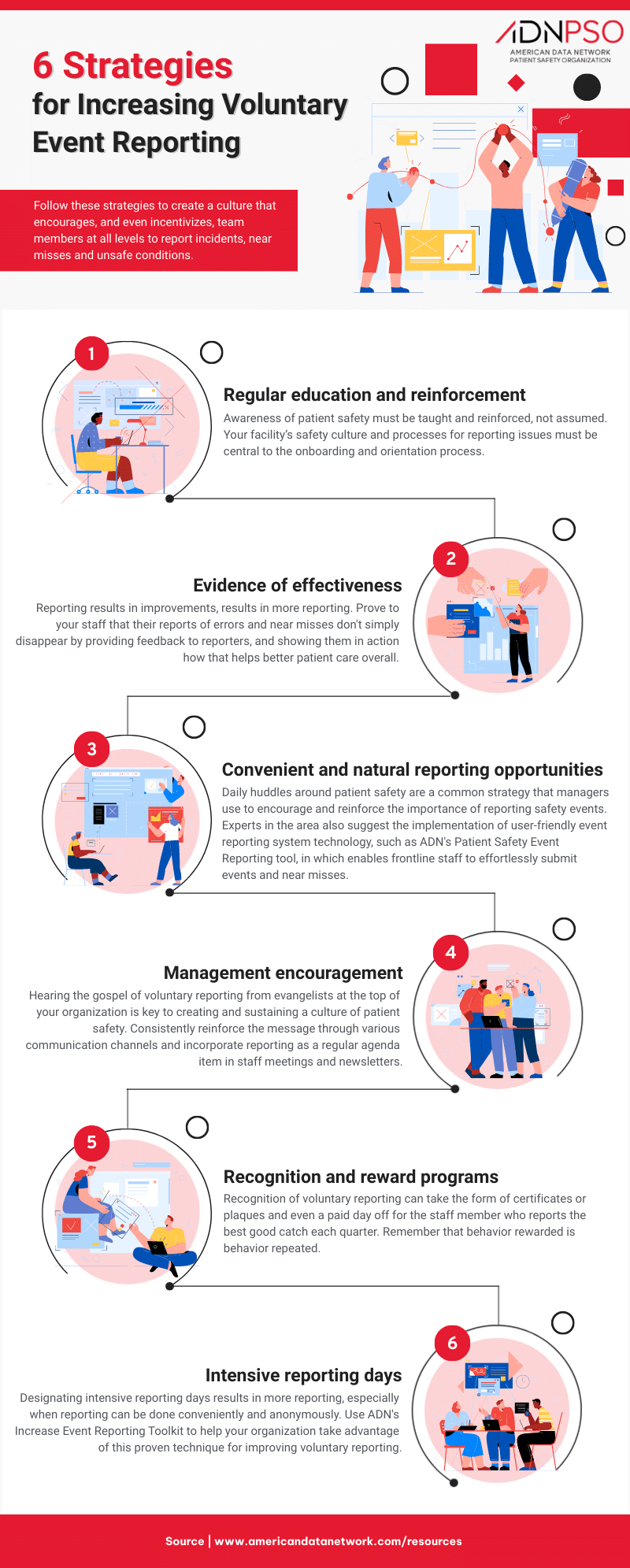
It’s counterintuitive but inescapable: To achieve the highest levels of reliability, High Reliability Organizations must defy human nature by eagerly embracing the evidence of failure. This article will suggest six strategies, and even more specific techniques, for creating a culture that encourages — and even incentivizes — team members at all levels to report incidents, near misses and unsafe conditions.
Encouraging and incentivizing reporting requires first understanding the reasons that team members may fail to do so. As the graphic below illustrates:
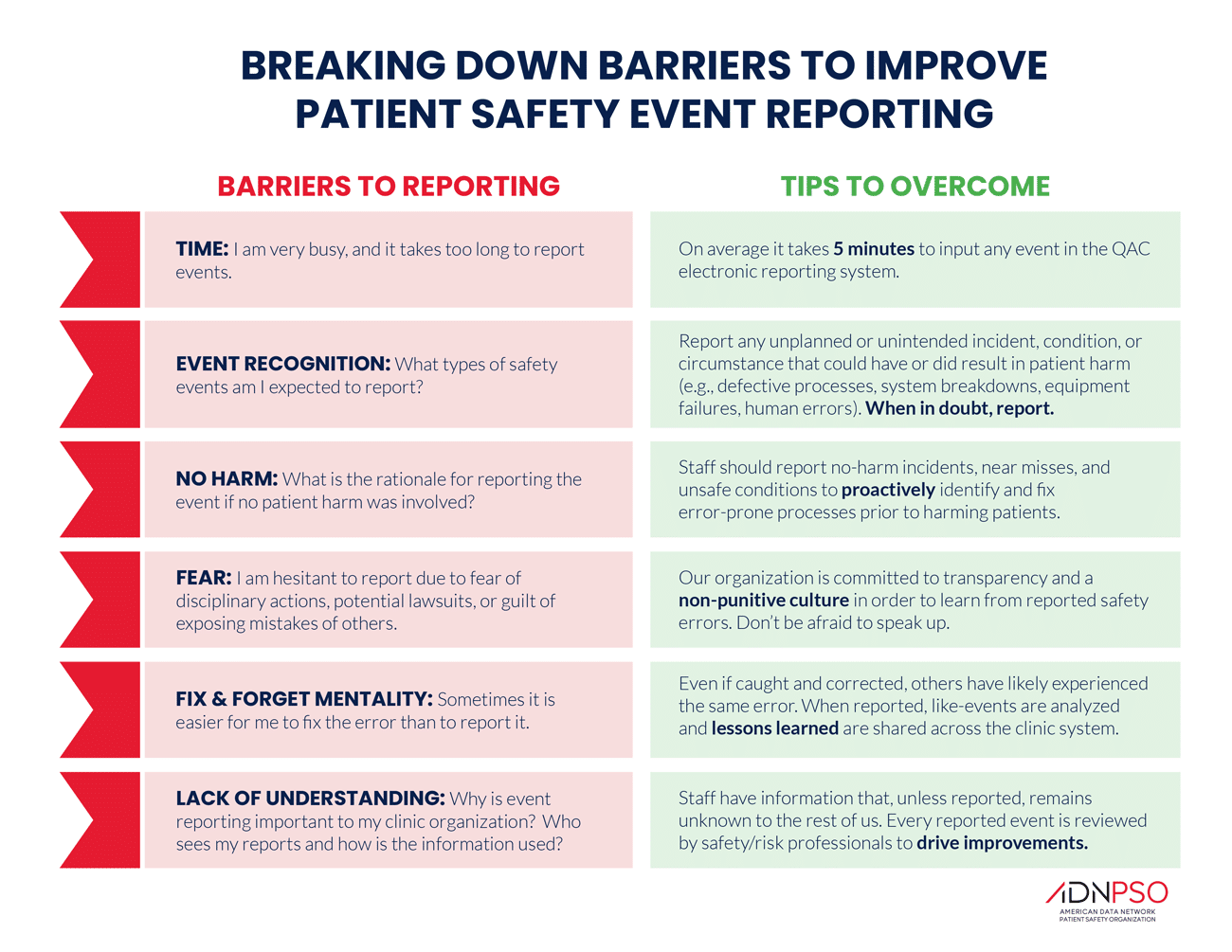

Awareness of patient safety as a science that must be taught and reinforced has been growing, but your hospital or clinic is an amalgam of patient care providers whose immersion in the mindset and culture of patient safety cannot be assumed. Your facility’s safety culture and processes for reporting issues must be central to the onboarding and orientation process.
As writer Susan Trossman described in a 2017 article in The American Nurse, cultural expectations like engaging in daily safety huddles and working collaboratively must be communicated to new hires and then reinforced in continuing training and routine communication. (Her article also describes an added benefit of intensive orientation, at least with nurses: higher rates of employee retention.)
Safety champions — engaged team members with specialized training — are a tried and true method of reinforcing your desired culture of safety, including normalizing routine reporting of events. Appointing champions per department or location is a great way to ensure the focus on reporting gets regularly communicated on the front lines.
Proving to your staff that their reports of errors and near misses don’t disappear into the ether creates a virtuous feedback loop: Reporting results in improvements, which results in more reporting. An analysis of data from more than 200,000 individuals in almost 1,000 hospitals concluded that prioritizing feedback to reporters is one of the most efficient ways to increase the likelihood that a patient safety event will be voluntarily reported. And this was especially true with the most serious patient safety events. (While you are at it, consider using language such as “safety report” rather than “incident report.”)
You may be familiar with “nudge theory,” the idea that desired behaviors can be fostered by making them more convenient. (This explains the candy bars in the checkout aisles of grocery stores — and Best Buy.) The desired outcome of voluntary reporting of patient safety events can also be nudged by creating convenient, natural reporting opportunities.
One common and effective strategy is the daily huddle, in which patient safety is the central agenda item for all team members. Periodic observation to make sure daily huddles are being used to encourage event and near-miss reporting is a good management technique. Consider adding the daily question: “How is the next patient going to be harmed?”
Anything that requires a lot of time and effort will always take a backseat to the urgency of patient care, so convenient reporting can also be encouraged with user-friendly reporting technology. This free Patient Safety Event Reporting Gap Analysis template can help you conduct a thorough evaluation of how well or poorly your existing tool or process accomplishes the necessary objectives of an event reporting system.
Hearing the gospel of voluntary reporting from evangelists at the top of your organization is key to creating and sustaining a culture of patient safety. These messages from leadership are an opportunity to dispel the fear of retribution from reporting events and instead help promote a just culture at your facility. ADN’s Increase Event Reporting Toolkit can help with templates for emails from senior leaders. Hanging posters reminding frontline staffers of the types of events they should report can keep the responsibility for reporting top of mind. (The toolkit also contains a poster template.)
Every communication channel in your organization is an opportunity for reinforcing the message: staff meetings, intranet, newsletters, etc. But it won’t get done unless someone is specifically tasked with adding safety to the to-do list. Staff meeting agendas and newsletters often feature standing items that carry over from one to the next; voluntary reporting should be one of those standing items.
Behavior rewarded is behavior repeated. Recognition of voluntary reporting through “good-catch campaigns” can take the form of certificates or plaques and even that most prized reward: a paid day off for the staff member who reports the best good catch each quarter.
If your state has a patient safety recognition program, be sure your good catches are entered. Whether your staff member is ultimately recognized statewide or not, knowing that their focus on safety has not been forgotten reinforces the original recognition.

It may seem counterintuitive in a culture that encourages reporting of incidents and near misses year-around, but designating intensive reporting days results in more reporting. Research published by the Journal of Patient Safety found that it works at all levels of an organization, especially when reporting can be done conveniently and anonymously.
Clinicians, staff members and patients in 10 family medicine clinics were encouraged to make routine reports during a 10-week study, but they were asked to report every error on five specific days. Their anonymous reports could come through a website, paper forms or a voice-activated phone system. During the 70-day study period, more than a third of the reports came on the five days that were designated for intensive reporting.
ADN’s Increase Event Reporting Toolkit includes an Intensive Reporting Day checklist and support materials to help your organization take advantage of this proven technique for improving voluntary reporting.
Then what?
As you implement new strategies and techniques to improve voluntary event reporting, you can track overall improvement and even compare your facility to other hospitals using ADN’s Patient Safety Event Reporting Rate Calculator. The calculator shows how far above or below average your event reporting rate is as well as suggested reporting rate improvement goals and more recommended strategies, tactics and tools based on your facility’s performance.
Falls Prevention Initiatives That Make a Difference
Falls in healthcare settings are a significant public health concern. They have consequences ranging from hip fractures to a heightened fear of falling. Not only do they increase bed time, but they can drastically reduce a patient’s quality of life.